
2 results
Are We Adequately Assessing Delirium? An Analysis Of Liaison Psychiatry Referrals
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S518-S519
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Delirium is characterised by an acute, fluctuating change in cognition, attention and awareness (Wilson et al. Nature Reviews 2020; 6). This presentation can make the diagnosis of delirium extremely challenging to clinicians (Gofton., Canadian Journal of neurological sciences. 2011; 38 673-680). It is commonly reported in hospitalised patients, particularly in those over the age of sixty five (NICE. Delirium: prevention, diagnosis and management. 2010).
ObjectivesOur aim is to identify which investigations and cognitive assessments are completed prior to a referral to the liaison psychiatry services in patients with symptoms of delirium.
MethodsReferrals (N = 6012) to the liaison psychiatry team at Croydon University Hospital made between April and September 2022 were screened. Search parameters used to identify referrals related to a potential diagnosis of delirium were selected by the authors. The terms used were confusion; delirium; agitation; aggression; cognitive decline or impairment; disorientation; challenging behaviour. Data was collected on the completion rates of investigations for delirium as advised by the NICE clinical knowledge summaries. Further data was gathered on neuroimaging (CT or MRI), cognitive assessment tools (MOCA/MMSE) and delirium screening tools (4AT/AMTS).
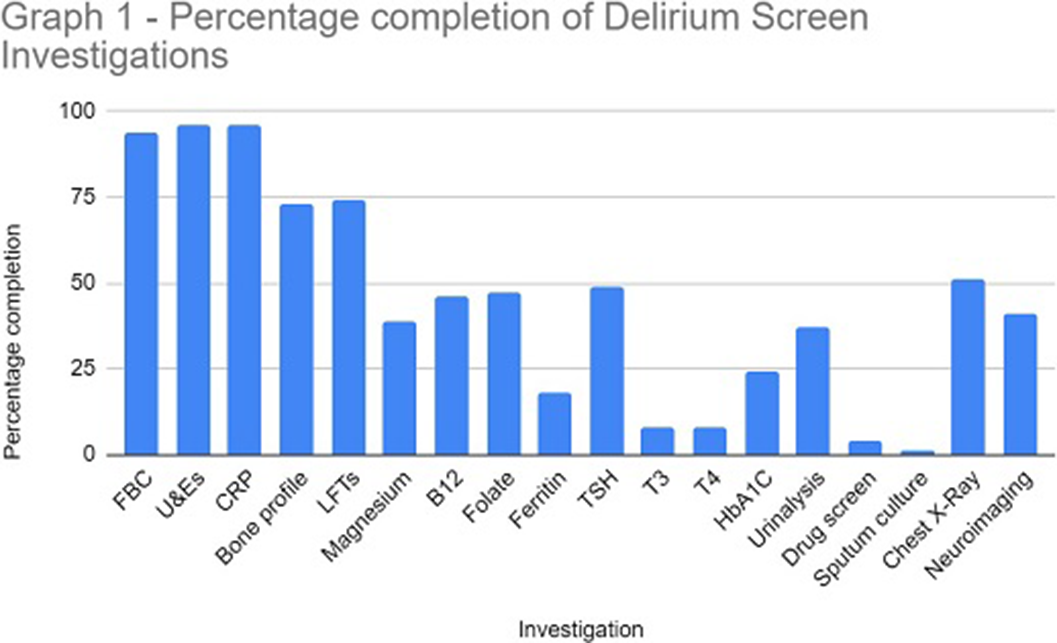
ResultsThe study sample identified 114 referrals (61 males and 53 females), with 82% over 65 years at the time of referral. In 96% of referrals, U&E and CRP were performed. Sputum culture (1%), urine toxin screen (4%) and free T3/4 (8%) were the tests utilised the least. Neuroimaging was completed in 41% of referrals (see Graph 1 for a full breakdown of results).
A formal cognitive assessment or delirium screening tool was completed in 32% of referrals. The AMTS and 4AT tools were documented for 65% and 24% respectively. A total of 19 referrals explicitly stated the patient was suspected to have dementia. A delirium screening tool was documented in 47% of these cases however, a formal cognitive assessment was documented in only 5% of these patients.
Following psychiatric assessment 47% of referrals were confirmed as delirium.
Image:
 Conclusions
ConclusionsOur data highlights the low level completion of the NICE recommended delirium screen prior to referral to liaison psychiatry. The effective implementation of a delirium screen and cognitive assessment is paramount to reduce the number of inappropriate psychiatric referrals in hospital and helps to identify reversible organic causes of delirium. This in turn will ensure timely treatment of reversible causes of delirium and reduce the length of hospital admission.
Disclosure of InterestNone Declared

Do psychiatric decision units make a difference? An analysis from a liaison psychiatry service in Greater London
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S70-S71
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
CAU (Clinical assessment unit) was developed at Croydon University Hospital (CUH) in conjunction with the South London and Maudsley (SLaM) mental health trust in response to the Covid19 pandemic to relieve pressure on services in A&E (Accident and Emergency) and to support the already existing need to provide a more clinically appropriate space for patients presenting to A&E with acute mental health concerns. The clinical model for the unit was developed with input from service users, SLaM, CUH and CCG (Clinical Commissioning Group); and was fully established in October 2021 within a month of conception. CAU is located within close proximity to A&E which is convenient and incurs no transfer cost. Similar units have been developed internationally to address similar concerns (Goldsmith et al 2021, Wiley online library 2021 12849)
ObjectivesTo evaluate the financial and clinical impact of the clinical assessment unit after one year in operation
MethodsThis is a cross sectional study, data was collected from EPJs Reports (SLaM’s patient data reporting system), excel spread sheet collecting data based on referrals to the service over the one-year period from 8/9/2021 – 5/10/2022. This included a trial period from September 2021 – October 2021 where the service was running at half capacity.
CAU is open to capacitous adults aged 18-65 presenting to A&E. Exclusion criteria: individuals conveyed by the police, those under MHA, on-going physical health concerns, diagnosis of learning disability with no primary mental health need, diagnosis of dementia and homelessness
Results3,322 patients were referred to the Liaison service and of those 402 or 12% of those patients to A&E were transferred to CAU
The 402 service users over the period of one year spent a total of 11, 351 hours in CAU
The main diagnosis of patient admitted to CAU fell into the diagnostic categories F30-39 43.5 %, and F60-69 27%.
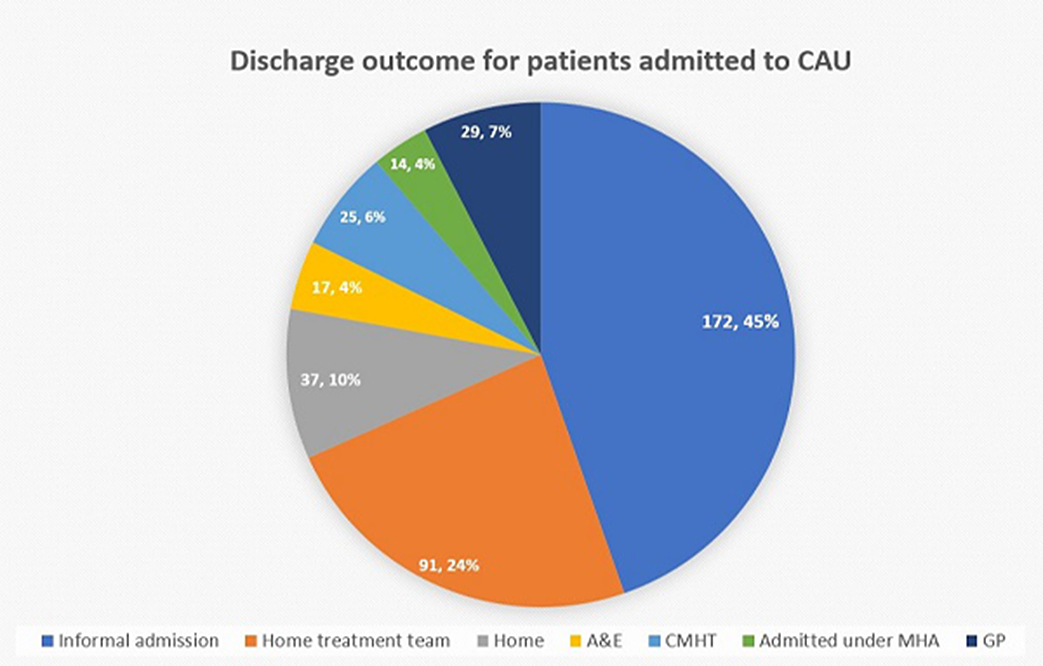
The majority of patients were admitted awaiting informal admission and 1/3 of plans for discharge destination were made on CAU. 10 % of patient were discharged on a least restrictive outcome, which has cost benefits for acute mental health trust. This one-year period showed cost saving of £462,112 for 24 hours stay in ED with support staff.
Image:
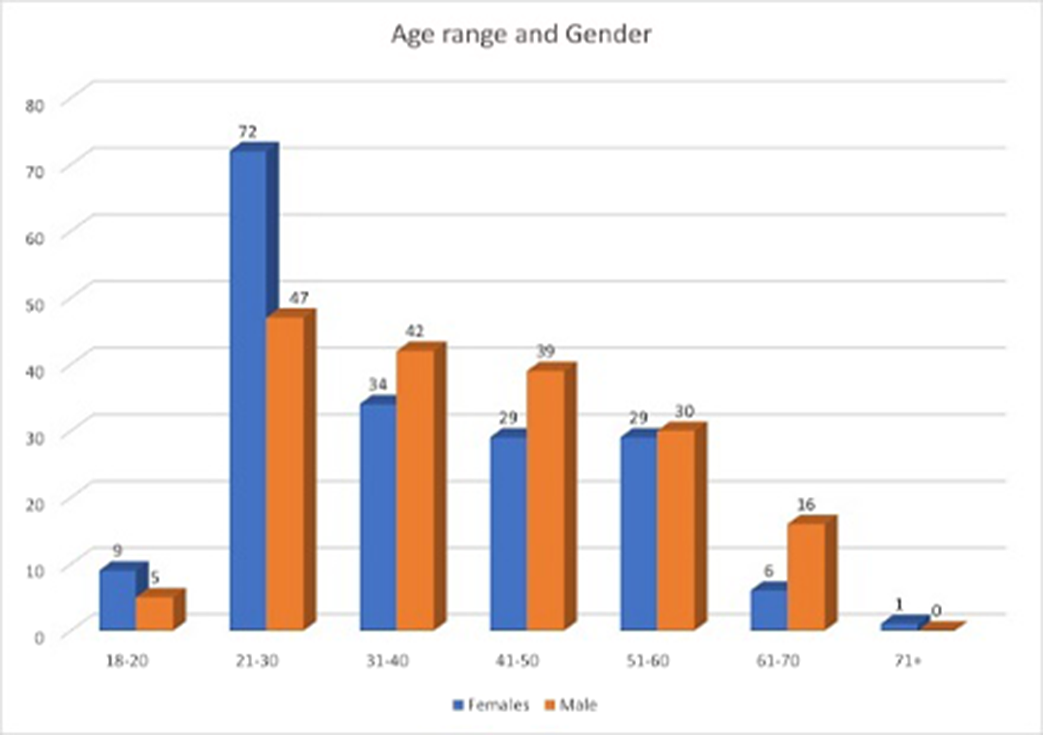
Image 2:
 Conclusions
ConclusionsCAU offers the opportunity to engage and re-assess service users to allow consideration of least restrictive options for on-going care. CAU has financial benefits in way of saving cost on time spent in ED awaiting review and cost for agency staff to provide 1:1 support.
The success of CAU has led to collaboration in the developpment of other acute services in London including that of the Recovery Space which offers community support for service users following discharge from hospital after an acute mental health crisis. Service user feedback has been positive and reflects the importance of the service and its suitability for its target group.
Disclosure of InterestNone Declared


